Free Nyc Pba 14 Form in PDF
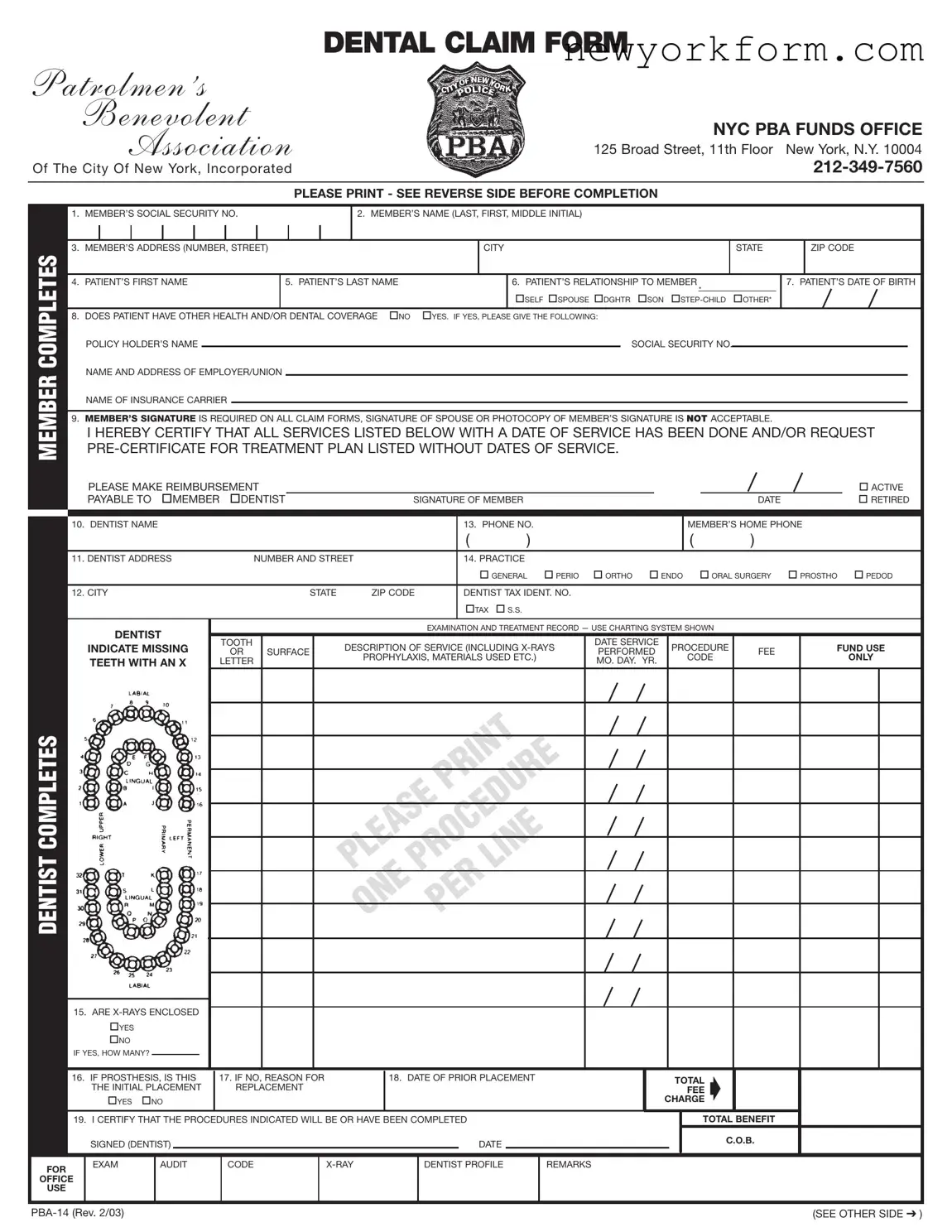
At the heart of dental health benefits for New York City's law enforcement officers is the NYC PBA 14 form, a crucial document designed to streamline the process of submitting dental claims within the context of the Patrolmen's Benevolent Association (PBA) funds. Situated at 125 Broad Street, the PBA Funds Office enables members and their families to navigate the complexities of dental care reimbursement through this meticulously structured form. Essential sections of the form include personal identification details like social security numbers and addresses, alongside critical information regarding the patient's relationship to the member, their coverage status, and detailed treatment records. A unique aspect of the NYC PBA 14 form is the necessity for a member's direct signature, underscoring the importance of authenticity and accountability in claims processing. Moreover, the inclusion of detailed instructions for both dental practitioners and members emphasizes the importance of pre-certification for specific treatments, highlighting the PBA's dedication to ensuring that its members receive pre-approved, necessary dental care without incurring unexpected expenses. The form, complete with directives for x-rays, study models for orthodontic claims, and periodontal charting, performs a dual role: it is both a claim form and a procedural guideline, ensuring clarity and efficiency in the delivery of dental benefits to New York's finest.
Nyc Pba 14 Sample
|
|
DENTAL CLAIM FORM |
PATROLMEN ’S |
|
|
|
BENEVOLENT |
NYC PBA FUNDS OFFICE |
|
ASSOCIATION |
|
|
125 Broad Street, 11th Floor New York, N.Y. 10004 |
|
|
Of The City Of New York, Incorporated |
|
|
|
|
|
|
|
|
|
PLEASE PRINT - SEE REVERSE SIDE BEFORE COMPLETION |
MEMBER COMPLETES
1. |
MEMBER’S SOCIAL SECURITY NO. |
|
|
|
2. MEMBER’S NAME (LAST, FIRST, MIDDLE INITIAL) |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
MEMBER’S ADDRESS (NUMBER, STREET) |
|
|
|
|
|
|
CITY |
|
STATE |
|
ZIP CODE |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
PATIENT’S FIRST NAME |
|
5. PATIENT’S LAST NAME |
|
|
|
6. PATIENT’S RELATIONSHIP TO MEMBER |
|
7. PATIENT’S DATE OF BIRTH |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SELF SPOUSE DGHTR SON |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
DOES PATIENT HAVE OTHER HEALTH AND/OR DENTAL COVERAGE |
NO |
YES. IF YES, PLEASE GIVE THE FOLLOWING: |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
POLICY HOLDER’S NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL SECURITY NO. |
|
|
|
|
|
||||
|
NAME AND ADDRESS OF EMPLOYER/UNION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
NAME OF INSURANCE CARRIER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
9. |
MEMBER’S SIGNATURE IS REQUIRED ON ALL CLAIM FORMS, SIGNATURE OF SPOUSE OR PHOTOCOPY OF MEMBER’S SIGNATURE IS NOT ACCEPTABLE. |
|
|
|
||||||||||||||||||||
I HEREBY CERTIFY THAT ALL SERVICES LISTED BELOW WITH A DATE OF SERVICE HAS BEEN DONE AND/OR REQUEST
|
|
PLEASE MAKE REIMBURSEMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACTIVE |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
PAYABLE TO |
MEMBER |
DENTIST |
|
SIGNATURE OF MEMBER |
|
|
|
|
|
|
DATE |
|
RETIRED |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10. DENTIST NAME |
|
|
|
|
|
|
|
|
13. PHONE NO. |
|
|
|
|
MEMBER’S HOME PHONE |
|
||||
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
( |
|
) |
|
|
|
|
11. DENTIST ADDRESS |
|
|
|
NUMBER AND STREET |
|
|
14. PRACTICE |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
GENERAL |
PERIO |
ORTHO |
ENDO |
ORAL SURGERY |
PROSTHO |
PEDOD |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
12. CITY |
|
|
|
|
|
STATE |
ZIP CODE |
|
DENTIST TAX IDENT. NO. |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
TAX |
S.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
DENTIST |
|
|
|
|
|
|
|
EXAMINATION AND TREATMENT RECORD — USE CHARTING SYSTEM SHOWN |
|
|
|
||||||||
|
|
|
|
TOOTH |
|
|
DESCRIPTION OF SERVICE (INCLUDING |
|
DATE SERVICE |
PROCEDURE |
|
FUND USE |
|||||||||
|
|
INDICATE MISSING |
|
|
|
|
|||||||||||||||
|
|
OR |
SURFACE |
|
PERFORMED |
FEE |
|||||||||||||||
|
|
|
|
|
|
PROPHYLAXIS, MATERIALS USED ETC.) |
|
|
CODE |
|
ONLY |
||||||||||
|
|
TEETH WITH AN X |
LETTER |
|
|
|
|
MO. DAY. YR. |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
COMPLETES |
|
||
|
|
LINE |
|
|
|
|
|
DENTIST |
PLEASEPROCEDURE |
||
ONE |
PER |
|
|
|
|
|
|
|
15. ARE |
|
|
|
YES |
|
|
|
NO |
|
|
|
IF YES, HOW MANY? |
|
|
|
|
16. IF PROSTHESIS, IS THIS |
17. IF NO, REASON FOR |
|
18. DATE OF PRIOR PLACEMENT |
|
TOTAL |
|||||||||||
|
|
|
THE INITIAL PLACEMENT |
|
REPLACEMENT |
|
|
|
|
|
|
|
FEE |
|||||
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
CHARGE |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
19. I CERTIFY THAT THE PROCEDURES INDICATED WILL BE OR HAVE BEEN COMPLETED |
|
|
TOTAL BENEFIT |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C.O.B. |
|
|
|
|
SIGNED (DENTIST) |
|
|
|
|
|
|
|
DATE |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR |
|
EXAM |
|
AUDIT |
|
CODE |
|
|
DENTIST PROFILE |
REMARKS |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
OFFICE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
USE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(SEE OTHER SIDE ) |
INSTRUCTIONS
PRECERTIFICATION IS REQUIRED FOR ALL CROWN AND BRIDGE, PROSTHETIC, ORTHODONTIC, AND PERIODONTIC WORK.
DENTIST:X-RAYS MUST BE SUBMITTED WITH ALL CLAIMS REQUESTING PRECERTIFICATION.
STUDY MODELS ARE ALSO REQUIRED FOR ALL
ORTHODONTIC CLAIMS.
PERIO CHARTING IS REQUIRED FOR ALL
PERIODONTIC CLAIMS
MEMBER:DO NOT ALLOW YOUR DENTIST TO COMMENCE ANY PROCEDURES WHERE PRECERTIFICATION IS REQUIRED UNTIL BOTH YOU AND YOUR DENTIST HAVE RECEIVED THE PRECERTIFICATION.OTHERWISE, YOU WILL BE LIABLE FOR PAYMENT OF SERVICES THAT MIGHT NOT BE APPROVED BY THE PLAN.
NOTE:ALL COMMUNICATIONS WITH THE FUNDS OFFICE MUST INCLUDE PATIENTS CLAIM NUMBER (WHEN KNOWN) OR MEMBERS SOCIAL SECURITY NUMBER.
IMPORTANT: FOR PROTECTION OF YOURSELF AND THE PBA FUNDS, PLEASE DO NOT SIGN BOX #9 ON THE FRONT OF THIS FORM UNTIL THOSE SERVICES ACTUALLY ARE PERFORMED OR THOSE REQUIRING PRECERTIFICATION HAVE BEEN
ALL CLAIMS SUBJECT TO REVIEW FOR COORDINATION OF BENEFITS
File Overview
| Fact | Detail |
|---|---|
| Form Name | PBA-14 Dental Claim Form |
| Usage | Used by members of the Patrolmen's Benevolent Association of the City of New York to submit dental claims. |
| Location | 125 Broad Street, 11th Floor, New York, N.Y. 10004 |
| Contact Information | Phone: 212-349-7560 |
| Key Requirement | Member's signature is mandatory on all claim forms; photocopies or signatures of spouses are not accepted. |
| Governing Law | Subject to New York State laws and regulations governing dental claims and insurance. |
Nyc Pba 14: Usage Guidelines
Filling out the NYC PBA 14 form, a dental claim form from the Patrolmen’s Benevolent Association, is a straightforward process when you follow the correct steps. This form is an essential document for members looking to claim dental expenses, ensuring that the process is conducted efficiently and properly. It’s crucial to complete this form accurately to avoid delays in your claim. Below are step-by-step instructions designed to guide you through each section of the form.
- Begin by entering the member’s Social Security number in the space provided for item 1.
- Fill out the member’s full name, including the last name, first name, and middle initial in the space provided for item 2.
- Write the member’s address, including the number, street, city, state, and zip code in the space provided for item 3.
- Enter the patient's first name in the space provided for item 4.
- Fill out the patient's last name in the space provided for item 5.
- Indicate the patient’s relationship to the member by selecting the appropriate option (e.g., self, spouse, daughter, son, step-child, other) for item 6.
- Enter the patient's date of birth in the space provided for item 7.
- If the patient has other health and/or dental coverage, check "Yes" and provide the policy holder’s name, Social Security number, name and address of employer/union, and the name of the insurance carrier in the spaces provided for item 8. If not, check "No".
- Enter the dentist’s name in the space provided for item 10.
- Fill out the dentist’s address, including the number and street, city, state, and zip code in the space provided for item 11.
- Provide the dentist’s phone number in the space provided for item 13.
- Select the practice type (general, perio, ortho, endo, oral surgery, prosth, pedod) by checking the appropriate box for item 14.
- Enter the dentist's tax identification number in the space provided for item 12.
- Indicate whether X-rays are enclosed by checking "Yes" or "No" and state how many for item 15.
- For prostheses, indicate if this is the initial placement or a replacement by checking "Yes" or "No" for item 16 and 17.
- Provide the date of prior placement if applicable for item 18.
- Enter the total fee charged in the space provided for item 19.
- The dentist must certify the completion or planned completion of the indicated procedures by signing in the space provided at the end of the form.
Before you fill out the form, please note that precertification is required for all crown and bridge work, prosthetic, orthodontic, and periodontic treatments. Additionally, your dentist must submit X-rays with all precertification requests, and for orthodontic claims, study models are also required. Do not commence any dental procedures requiring precertification until both you and your dentist have received the precertification to avoid being liable for the payment of services that might not be approved. Remember, your completed form should include all necessary documentation as indicated, ensuring that each step is followed correctly to facilitate a smooth review process by the PBA Funds Office.
FAQ
What is the NYC PBA 14 form used for?
The NYC PBA 14 form is utilized for submitting dental claim requests for members of the Patrolmen’s Benevolent Association (PBA) of the City of New York, Incorporated. It allows members to apply for reimbursements for dental services received, covering various procedures including preventive, basic, and major services. The form must be accurately completed and submitted following the guidelines detailed on the form to ensure the claim is processed efficiently.
Who needs to complete the NYC PBA 14 form?
Both the member receiving dental services and the dentist providing the services are required to fill out sections of the NYC PBA 14 form. Members must provide their personal and insurance information, certify that the services have been performed or are needed by signing the form, and ensure that any necessary precertification has been obtained. Dentists are responsible for describing the services provided, including any procedures and treatments, along with attaching any necessary documentation such as x-rays or study models for orthodontic claims.
Is it necessary for the member to sign the NYC PBA 14 form?
Yes, it is crucial for the member to sign the NYC PBA 14 form. The signature certifies that the listed dental services have been performed or are requested. Importantly, a member’s signature is mandatory on all claim forms, and neither a spouse's signature nor a photocopy of the member's signature is acceptable. This step is vital for the processing and approval of the claim.
Are there specific requirements for submissions concerning prostheses or orthodontic, crown, and bridge work?
Yes, specific requirements apply to these types of dental work. Precertification is required for all crown and bridge work, prosthetic, orthodontic, and periodontic treatments. Additionally, x-rays are required for all claims that request precertification, and for orthodontic claims, study models are also necessary. For periodontic claims, periodontal charting is required. Members should refrain from allowing their dentist to start any treatments requiring precertification until both the member and dentist have received precertification approval to avoid being liable for payments of services not approved by the plan.
What happens if the form is not signed by the member or if pre-certification is not obtained?
If the NYC PBA 14 form is not properly signed by the member or if the necessary precertification is not obtained for certain procedures, the claim may be denied or delayed. This could result in the member being responsible for the full cost of the dental services. It is essential for the member to ensure that all required signatures are in place and that precertification requirements are fulfilled before undergoing specific dental treatments.
Can a claim be submitted if the patient has other health or dental coverage?
Yes, a claim can be submitted if the patient has other health or dental coverage. However, it is important to provide the details of the additional coverage on the NYC PBA 14 form, including the policy holder’s name, social security number, the name and address of the employer or union, and the name of the insurance carrier. This information is necessary for the coordination of benefits, ensuring that all benefits available to the patient are appropriately applied.
How should a member submit the NYC PBA 14 form?
After accurately completing the NYC PBA 14 form and obtaining any required documentation and signatures, the member should submit the form to the PBA Funds Office, located at 125 Broad Street, 11th Floor, New York, N.Y. 10004. It is advisable to keep a copy of the completed form and any accompanying documents for personal records. Furthermore, members should ensure that all communications with the funds office include either the patient's claim number (when known) or the member's social security number for accurate processing of the claim.
Common mistakes
When filling out the NYC PBA 14 form, individuals often overlook key details that are vital for the submission process, leading to common mistakes. These errors can delay or even prevent the successful processing of dental claims. Recognizing and avoiding these mistakes ensures smoother transactions with the Patrolmen's Benevolent Association's Funds Office.
Firstly, a frequent oversight is the incorrect or incomplete filling of the member’s Social Security Number. This number is essential for identifying the member within the system, and any error can lead to significant delays. Secondly, many individuals fail to print their information clearly, which is crucial since illegible handwriting can cause misinterpretation of vital data. The member’s signature requires special attention; a common mistake is the submission of a form with a missing or invalid signature, as photocopies or spouse signatures are not acceptable.
Additionally, people often overlook the importance of indicating whether the patient has other health or dental coverage. Providing complete and accurate information in this section is necessary for proper coordination of benefits. Another related mistake is to begin treatments requiring precertification without confirmation. Starting any procedure without both the member and the dentist receiving precertification paperwork from the PBA Funds Office exposes the member to potential financial liability for services not approved by the plan.
Errors related to the dentist’s information are also common. It's crucial to ensure that all details, including the dentist's name, address, and tax identification number, are filled out accurately. Moreover, when documenting the examination and treatment record, every section, including descriptions of service, dates, and fees, must be completed meticulously. Here, a frequent mistake is failing to indicate the necessity for accompanying materials, such as x-rays or periodontal charting, which are mandatory for precertification in certain cases.
In the realm of additional documentation, forgetting to enclose necessary x-rays or providing unclear reasons for prosthesis replacement counts as mistakes as well. Documents supporting the claim or required for precertification must be attached as specified in the form instructions. Finally, an often overlooked but crucial detail is ensuring that all procedure codes are accurately entered. Incorrect or missing codes can lead to claim rejection or processing delays.
Below is a summary of the common mistakes made when completing the NYC PBA 14 form:
- Inaccurately filling out the member’s Social Security Number.
- Legibility issues due to unclear printing of information.
- Submitting the form with an invalid or missing member's signature.
- Omitting details about other health or dental coverage.
- Commencing treatments requiring precertification without the necessary approval.
- Misrepresenting or incorrectly entering the dentist’s information.
- Failing to complete every section of the examination and treatment record accurately.
- Neglecting to enclose necessary x-rays or supply required documentation.
Avoiding these mistakes not only facilitates a smoother claims process but also ensures that members receive the benefits to which they are entitled without unnecessary delay.
Documents used along the form
When dealing with the complexities of dental care management, particularly through the New York City Patrolmen's Benevolent Association (NYC PBA), the PBA 14 Dental Claim Form stands as a primary document for members seeking reimbursement or direct billing for dental services. Yet, this form often doesn't act alone in the journey of managing dental claims, benefits, and treatments. To navigate through this process effectively, members find themselves needing an array of additional forms and documents, each serving its unique role in ensuring comprehensive care and financial management.
- Pre-Treatment Estimate Form: Often used in conjunction with the PBA 14 form for procedures requiring pre-certification, this form provides detailed information about the proposed dental work, estimated costs, and necessity of the procedure, allowing for financial planning and insurance approval before the treatment begins.
- Annual Benefits Statement: This document provides a yearly overview of the dental benefits used by the member and remaining balances, helping members to track their dental insurance utilization and plan for future dental needs.
- Coordination of Benefits Form: When a patient has dental coverage under more than one insurance plan, this form is essential. It helps to determine the order in which the policies pay out their benefits, ensuring that the coverage is maximized and the submission to secondary insurances is streamlined.
- Insurance Appeal Form: If a claim is partially or fully denied, this document is utilized to contest the insurance company's decision. It allows members to provide additional information or clarification that could impact the insurer's review and potential reversal of their decision.
- Change of Beneficiary Form: This form allows members to update or change the beneficiary(ies) for any insurance payout or benefits. It's crucial for ensuring that benefits are directed according to the member's current wishes.
- Dental History Form: New patients or those seeing a specialist for the first time often need to complete this form, which provides the dentist with a comprehensive view of the patient's dental and medical history, aiding in personalized and effective treatment planning.
- Consent Forms: For certain procedures, especially those that are invasive, require sedation, or pose significant risks, written consent forms are necessary. These documents ensure that patients have been informed about the risks, benefits, alternatives, and have agreed to the procedure.
Together with the NYC PBA 14 form, these documents form a cohesive toolkit that empowers members to actively participate in their dental care management, from pre-treatment to post-care financial responsibilities. Understanding and utilizing these forms and documents can significantly ease the process of navigating through dental treatments, ensuring both health and financial well-being are managed with care and precision.
Similar forms
The American Dental Association (ADA) Dental Claim Form is remarkably similar to the NYC PBA 14 form in structure and purpose. Both forms are designed for the submission of dental claims to ensure that patients receive the appropriate reimbursement for dental services rendered. Like the NYC PBA 14 form, the ADA form collects detailed information about the patient, the subscriber, the dental services provided, including dates, and charges for the treatment, and requires the dentist's certification that the services have been completed. Additionally, both documents request dentist and practice information, such as tax identification numbers and addresses.
The Health Insurance Portability and Accountability Act (HIPAA) Patient Authorization Form shares a crucial similarity with the NYC PBA 14 form in terms of confidentiality and privacy. Although primarily focused on authorizing the disclosure of individual health information, the HIPAA form, like the PBA 14, contains provisions to protect patient data. Both documents are designed with the understanding that sensitive personal and health information is being handled, necessitating signatures to validate the authenticity of the information provided and to ensure that it is not disclosed without proper authorization.
The Employee Dental Service Claim Form used by many corporate dental plans also bears a resemblance to the NYC PBA 14 form. It is used by employees to claim dental benefits provided by their employer's insurance plan. Similar to the NYC PBA 14 form, it gathers comprehensive details about the patient's treatment, dental professional, and costs incurred. Both forms are instrumental in the process where employees or beneficiaries submit claims to receive coverage or reimbursement for dental services.
The Flexible Spending Account (FSA) Reimbursement Claim Form, commonly used by individuals with FSA accounts to request reimbursements for eligible health expenses, has parallels with the NYC PBA 14 form. While it covers a broader range of health services beyond dental, the process of submitting claims, providing proof of service, and detailing expenses is akin to the structure seen in the PBA 14 form. Each requires detailed information about the service, the provider, and the cost to process the claim efficiently.
The Workers' Compensation Dental Claim Form is another document that shares similarities with the NYC PBA 14 form. This form is specifically used for dental injuries sustained in the workplace and requires detailed documentation of the injury, treatment, and expenses, mirroring the information needed on the PBA 14 form. However, it uniquely focuses on the causality between the workplace and the dental injury, something not required in the general dental claims process.
Medicaid Dental Claim Forms, used by patients covered under Medicaid for submitting dental claims, resemble the NYC PBA 14 form in their aim to facilitate reimbursement for covered dental services. Both sets of forms necessitate detailed information on the service provided, including patient and provider details, to ensure that claims are processed according to the specific coverage policies. Furthermore, they both play a pivotal role in providing access to necessary dental care for eligible individuals or groups.
The Medical Expense Reimbursement Form, part of Health Reimbursement Arrangements (HRA) or other medical savings accounts, also shares a resemblance with the NYC PBA 14 form. Although broader in scope, covering a wide range of medical expenses, the fundamental purpose of documenting medical transactions for reimbursement purposes links them closely. Both require detailed documentation of services received, including provider information and the cost of services, to validate claims for reimbursement.
The Dental Pre-Authorization Form, often used to obtain approval for specific dental procedures before they occur, bears a functional similarity to the NYC PBA 14 form, particularly in its role in the dental insurance process. While the pre-authorization form focuses on obtaining upfront approval, and the NYC PBA 14 form deals with claiming reimbursement after services have been rendered, both are essential in the process of managing and limiting the financial risks associated with dental care. Each requires detailed treatment plans, including necessary dental services and estimated costs.
Dos and Don'ts
When it comes to filling out the NYC PBA 14 Dental Claim Form, accuracy and attention to detail are crucial for a successful submission. Here are six key dos and don'ts to guide you through the process:
Dos:- Read the instructions carefully before starting. The reverse side of the form contains valuable information on how to complete it properly.
- Ensure all personal information is accurate and legible, including the social security number, name, address, and relationship to the member.
- For treatments that require pre-certification, such as crowns, bridges, or orthodontic work, make sure you have received pre-certification before commencing the procedures.
- Include all necessary documentation, such as X-rays or periodontic charts, especially for claims requesting pre-certification.
- Sign the form personally in box #9. Remember, photocopies of signatures or signatures of spouses are not accepted.
- Make sure the dentist fills in all relevant sections accurately, including their name, address, tax identification number, and details of the treatment provided.
- Do not sign box #9 on the front of the form until the services are actually performed or those requiring pre-certification are filled in by the dentist, for the protection of both yourself and the PBA funds.
- Avoid letting the dentist start any pre-certification required procedures until you both have received pre-certification approval. Otherwise, you might be responsible for payments not covered by the plan.
- Do not leave any required fields blank. Incomplete forms can result in delays or denial of the claim.
- Avoid making changes or using correction fluid on the form. If you make an error, it's better to start with a new form to ensure clarity and prevent processing errors.
- Do not forget to include the patient's claim number or the member's social security number in all communications with the funds office. This is essential for tracking and processing your claim.
- Do not ignore the coordination of benefits review. All claims are subject to this review, which could affect the reimbursement amount.
By following these guidelines, you can ensure that your NYC PBA 14 Dental Claim Form is filled out correctly and processed without unnecessary delays, making the path to receiving your benefits smoother and more straightforward.
Misconceptions
Many people have misconceptions about the NYC PBA 14 form, which is essential for filing dental claims through the Patrolmen's Benevolent Association Funds Office. Understanding these misconceptions can help ensure that members accurately complete their forms and receive the benefits they're entitled to. Here are eight common misconceptions explained:
- Only the dentist is responsible for completing the form. While it might seem that the form is purely for dental professionals to fill out, members also have sections they must complete themselves. This includes personal information and details about additional insurance coverage.
- Any family member can sign the form in place of the member. This is not true. The form explicitly requires the signature of the member; a spouse's signature or a photocopy of the member's signature is not acceptable.
- Pre-certification is only a recommendation. In fact, pre-certification is mandatory for all crown and bridge work, prosthetic, orthodontic, and periodontic treatments. This is a critical step to ensure coverage for these procedures.
- X-rays are only sometimes required when submitting a claim. The form states that x-rays must accompany all claims requesting pre-certification. Moreover, for orthodontic claims, study models are also a requirement.
- The form is only for use by members of the NYC PBA. While it is tailored for members of the Patrolmen's Benevolent Association of the City of New York, the form serves as a claim document for dental services covered by their plan. Family members under their coverage also use this form for dental claims.
- All dental procedures are covered without approval. This is not accurate. Some procedures require pre-certification, and starting them without this approval could leave the member liable for the costs. It's crucial to receive pre-certification to ensure coverage.
- Members should sign the form before the service is performed. One should only sign the form after the service has been performed or for services requiring pre-certification that have been filled in by the dentist. This ensures that only completed or approved procedures are claimed.
- It doesn't matter when you submit the form as long as it's within the same year. Timely submission of the form is crucial. Delaying the submission can lead to delays in reimbursement or denial of the claim altogether. Members should ensure they and their dentists complete and submit claims promptly after services are rendered.
Understanding and addressing these misconceptions about the NYC PBA 14 form can streamline the process of filing dental claims, ensuring that members of the Patrolmen's Benevolent Association efficiently receive their dental benefits.
Key takeaways
Filling out the NYC PBA 14 Dental Claim Form correctly ensures timely processing of dental claims for members of the Patrolmen's Benevolent Association. This guide highlights five key takeaways to remember when completing and using the form.
- Complete All Relevant Sections Carefully: The form requires detailed information, including the member’s Social Security number, member and patient names, relationships, and addresses. Ensure all information is accurate and legible to avoid delays in claim processing.
- Pre-Certification Requirements: For certain types of dental work, such as crown and bridge, prosthetic, orthodontic, and periodontic treatments, pre-certification is mandatory. Do not commence any procedures that require pre-certification until receiving approval, or you may be liable for payment.
- Submission of Supporting Documents: When seeking pre-certification or filing a claim, attaching X-rays or study models (for orthodontic claims) is required. These supporting documents help in the assessment and approval of your claim.
- Signature Requirements: A unique aspect of this form is that a photocopy of the member’s signature is not accepted. The member, not the spouse or another individual, must sign the form. This is a critical step in the claim submission process.
- Coordination of Benefits: If the patient has other health or dental coverage, this must be disclosed on the form. Including details of additional coverage assists in the coordination of benefits and might impact the reimbursement outcome.
By paying attention to these key points, members can facilitate efficient processing of dental claims, ensuring that they and their dependents receive the benefits entitled to them under the NYC PBA plan.
Common PDF Documents
Do You Have to Pay Taxes on Estate Inheritance - Empowers estates with the means to clarify the decedent's residential intent and ties to New York State.
Nyc Food Service Establishment Permit - Applicants aiming for food service roles within New York State public entities must navigate the OC-APP #4 20-484 form, facilitating their examination entry.
Form 351 - The instructions within help disability retirees in reporting their personal service income, distinguishing between public and private sector earnings.